-
 WelcomeELSaad PharmaLeading, world-class branded healthcare company
WelcomeELSaad PharmaLeading, world-class branded healthcare company -
 WelcomeELSaad PharmaLeading, world-class branded healthcare company
WelcomeELSaad PharmaLeading, world-class branded healthcare company
www.elsaad.com
ELSaad Pharma leading, world-class branded healthcare company.
ELSaad Pharmaceuticals is a leading Syrian Pharmaceutical company established in the beginning of 1995 with an aim to serve medical association and Patient with best quality medicines.
ELSaad Pharmaceuticals is a leader in the Antibiotics and Respiratory segments, and has a strong presence in cardiovascular, Analysis, Urology, Dermatology, General and Local Anesthetic and Anti-Diabetics segments.
ELSaad which has been in the Pharma business for just 18 years has grown through an aggressive strategy of successfully managed acquisitions and alliances. Our portfolio of over 110 products are marketed by a large network of publicity representatives of doctors and pharmacists outnumber the 200 in various Syrian governorates.This is one of the strongest distribution channels in the industry.


www.elsaad.com
New Products

{kind=link}
{kind=link}
{kind=link}

{kind=link}

{kind=link}

{kind=link}

www.elsaad.com
GET IN TOUCH
www.elsaad.com
www.elsaad.com
Library of articles

Overview Sleep disorders are conditions that result in changes...
— also known as a seizure disorder —...

Overview Rosacea (roe-ZAY-she-uh) is a common skin condition that...
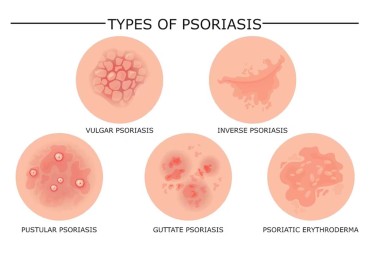
Overview Psoriasis is a skin disease that causes a...

Overview Acne is a skin condition that occurs when...

Overview Heart failure — sometimes known as congestive heart...